7-hydroxymitragynine (7OH) is a naturally occurring compound in the kratom plant, classified as a partial mu-opioid receptor agonist with unique pharmacodynamics. Unlike traditional opioids or synthetic analogs, 7OH displays a fast onset, minimal euphoric profile, and reduced respiratory depression. Despite this, it is under increasing scrutiny by policymakers considering potential scheduling. This article challenges that stance using community data, pharmacological profiles, peer-reviewed studies, and real-world outcomes.
7OH binds to the same receptors as morphine but with a different downstream signaling cascade. This results in G-protein-biased signaling, associated with reduced side effects compared to beta-arrestin pathways implicated in traditional opioids (Kruegel et al., 2016).
7OH occurs naturally in kratom leaves. Efforts to classify it as a synthetic compound misrepresent its origin and could mislead public opinion. According to NIH research (PMC6598155), 7OH arises metabolically from mitragynine both in vivo and in vitro.
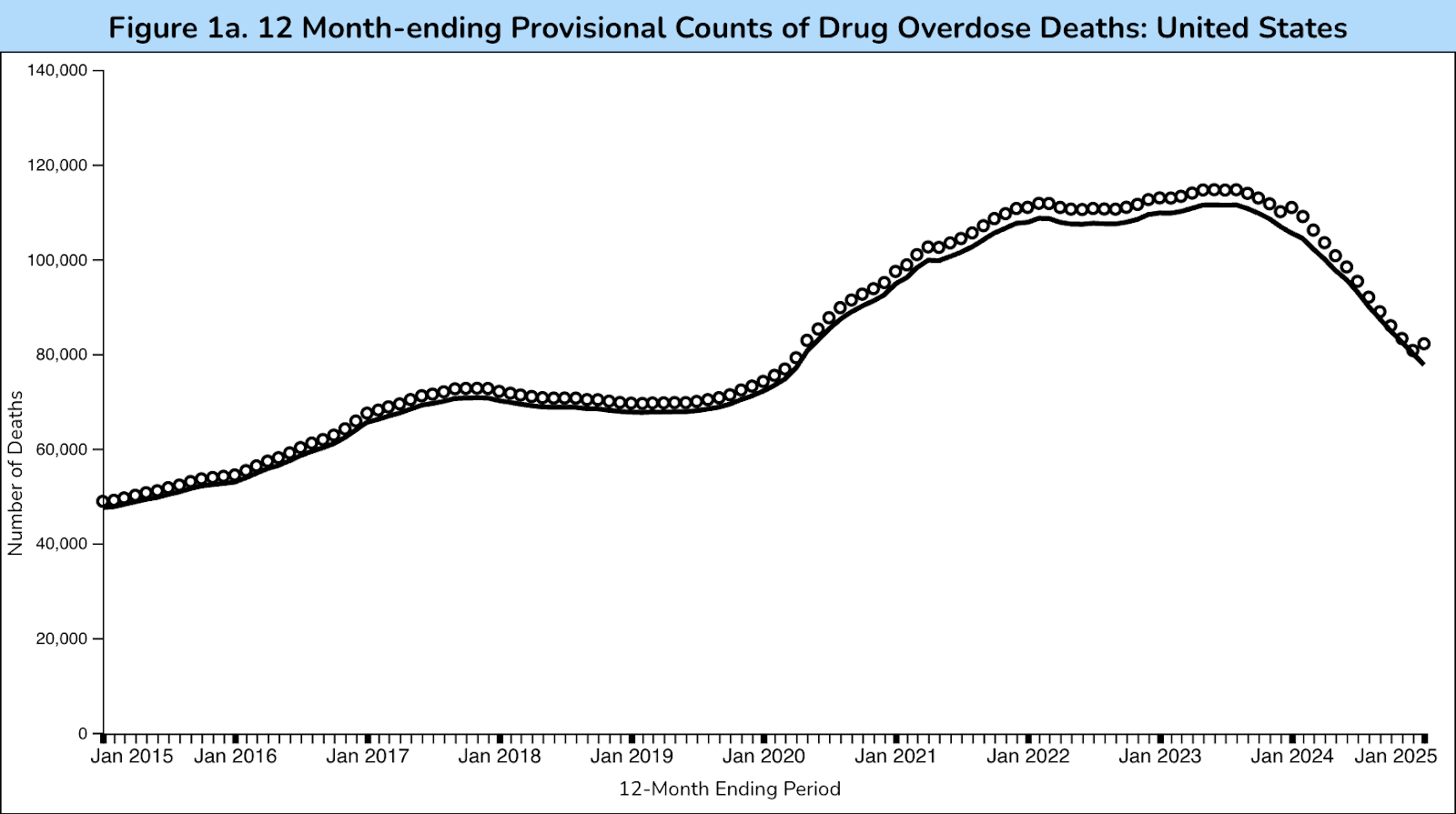
The CDC reported a 24% drop in drug overdose deaths between Sept 2023–Sept 2024 (CDC Report). While causation isn’t proven, the increase in 7OH usage coincides with this decline. Users report tapering off opioids without transitioning to equally addictive substances.
“7OH has done more for me than Suboxone has. With fewer side effects.” — Cody G.
In a preliminary dataset (N=122) collected via community survey in 2025, 84% reported reduced reliance on prescription medications after 30 days of consistent 7OH use. 68% said they experienced improved daily functionality without experiencing sedation.
Current Landscape:
If 7OH is scheduled without clear abuse metrics, it sets a precedent for banning any naturally occurring alkaloid with opioid-like receptor binding—even when the risk profile is significantly lower.
Further, in a recent review of plant-based compounds for pain and mood disorders, the National Center for Complementary and Integrative Health (NCCIH) acknowledged a growing interest in botanicals that show receptor selectivity and low abuse liability—criteria that align with 7OH.
Scheduling 7OH would punish low-risk users and undermine harm-reduction efforts supported by real-world evidence. The compound’s effects are distinct from synthetic opioids, and its role as a functional, non-intoxicating support tool warrants further independent clinical trials—not prohibition.
Lawmakers must ask:
If we are to move forward in evidence-based public health, 7-hydroxymitragynine deserves regulation—not eradication.
This article contains anonymized personal accounts voluntarily provided by individuals who participated in independent harm-reduction research efforts. All testimonials have been stripped of personally identifiable information in strict accordance with de-identification standards. No protected health information (PHI) is stored, transmitted, or published. This content is presented solely for informational and educational purposes and does not constitute medical advice, diagnosis, or treatment. The information herein complies with applicable U.S. privacy laws, including HIPAA, under exemptions for de-identified data used in public health and ethnographic research contexts.